In this review we are going to discuss what Popliteal Artery Entrapment Syndrome (PAES) is,...
Exercise-induced leg pain (EILP) is an umbrella term to describe pain in the leg as a result of exercise/physical activity. Symptoms may arise and worsen during physical activity or may present at rest and be manageable during activity. Symptoms other than pain may include burning, pins and needles, numbness, tightness, fatigue.
This paper by Bosnina et al. (2023) has categorised common EILP's to aid diagnosis:
- 1) Muscular origin pain, such as chronic exertional compartment syndrome (CECS) and myofascial tears
- 2) Bony origin pain , such as medial tibial stress syndrome (MTSS) and tibial stress fracture (TSF)
- 3) Nerve entrapment or compression pain, such as superficial peroneal nerve entrapment syndrome (SPNES)
- 4) Radicular pain or radiculopathy
- 5) Vascular origin - vascular origin due to temporary compression of either an artery or a vein, such as popliteal artery entrapment syndrome (PAES)
- 6) Muscle disorders, such as McArdle’s syndrome (metabolic disorder leading to muscle cramps and fatigue.
- 7) accessory or low-lying soleus muscle syndrome (ALLSMS) (also known as ASM) - anatomical variant characterised by an additional distinct muscle encountered along a normal soleus muscle.
Differentials:
- CECS - increased pressure in the lower leg compartment causing severe pain, tightness, and paraesthesia. The anterior compartment is most affected, can be both unilateral and bilateral. Tightness occurs in the affected compartment due to an increase in intramuscular pressure and subsequent symptoms. Key subjective markers include a pain pattern of pain that worsens with exercise and then resolves within minutes of rest and no pain at rest.
- MTSS - periostitis causing diffuse pain for months to years at the distal posteromedial border of the tibia, which can be unilateral or bilateral. Pain pattern shows pain during that arises during activity and can last for a few hours to days per episode. The
mechanism is subcutaneous periostitis associated with altered biomechanics of the lower limb, training errors and increased training intensity. The diagnosis of MTSS was based mainly on a history of persistent, cumulative pain that does not immediately
cease after stopping activity and may persist between a few hours and a few days. Occasionally in the early phases, pain will improve with running. - Tibial stress fracture - is defined as cortical or full bone fracture causing localised excruciating pain both at rest
and with weight-bearing activity with night pain. The mechanism is an imbalance between osteoblast (bone remodelling) and osteoclast (bone breakdown) activity leading to bone breakage due to overtraining, overuse, and repeated overloading. Focal pain during exercise and on palpation and positive imaging findings are key diagnostic findings as well as positive hop tests. - Superficial peroneal nerve entrapment syndrome - mechanical compression of the superficial peroneal nerve causing moderate to severe pain, paraesthesia, numbness, and the feeling of a ‘restless leg'. Symptoms occur with activity and are relieved with a variable period of rest. The mechanism is scarring/entrapment around the opening of the fascia where the nerve becomes a cutaneous sensory nerve supplying the dorsum of the foot. History of non-specific exertional neurological type of pain over the anterior compartment, accompanied by weakness, positive Tinel’s test, and altered sensation.
- Myofascial tear - single event causing a tear within the myofascial causing pain with activity as the main symptom and can be severely disabling.
- Lumbar Radicular pain or radiculopathy - mechanical compression of a nerve root at the level of the spinal cord causing sharp pain (radicular pain) which radiates down the legs with paraesthesia and numbness (radiculopathy). Loss of muscle strength may also be present (radiculopathy). Diagnosis revolves primarily around the history of radiating pain and neurological symptoms which are correlate with special testing and imaging.
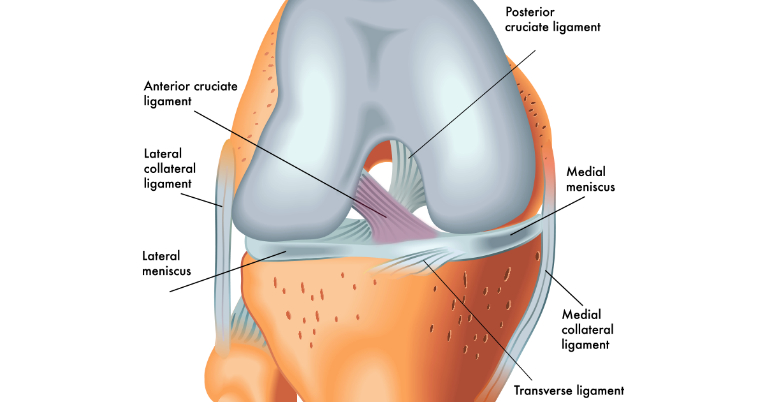
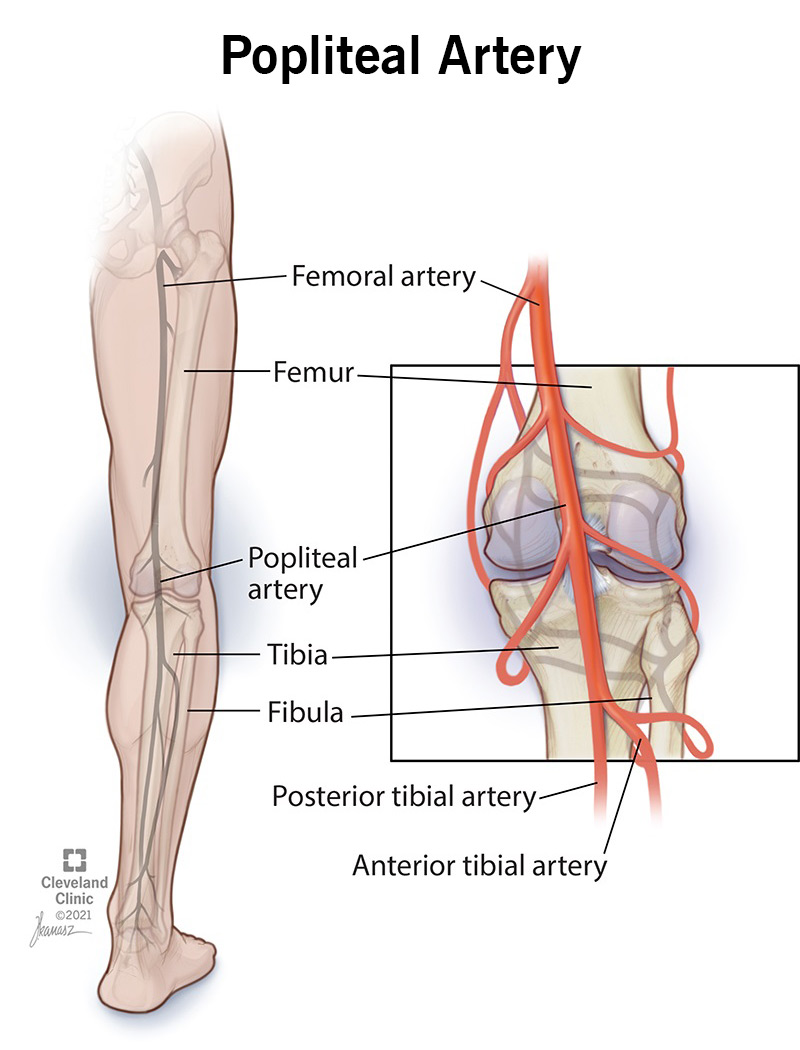
- ** PAES - caused by extrinsic compression of the popliteal artery, caused by the surrounding musculo-tendinous structures with the most frequent cause being the medial head of the gastrocnemius muscle, which causes intermittent claudication.
- McArdle's syndrome - autosomal recessive metabolic myopathy causes pain, tightness, swelling, malaise, and lethargy. McArdle’s syndrome diagnosis is confirmed by resting creatine kinase (CK) followed by 3 consecutive post-exercise CK and muscle biopsy
- Accessory/low-lying soleus muscle syndrome - space occupying mass which can cause nerve compression which mimics tarsal tunnel syndrome and can also cause increase in the intercompartmental pressure mimicking CECS. Other symptoms that may be attributed to impingement on neurovascular structures and paraesthesia and numbness affecting the plantar aspect of the foot. It occurs at the superficial posterior compartment and can be unilateral or bilateral and more common in young active adults. Diagnosis relied heavily on the absence of traumatic history, the lack of major presenting symptoms and the presence of anatomical variation on examination. Accessory and low-lying soleus muscles are present as normal anatomical variations in many asymptomatic subjects. A significant increase in intensity and exercise workload, in some cases, may lead to pain and disability.
References:
Bosnina et al. (2023) Developing a diagnostic framework for patients presenting with Exercise Induced Leg Pain (EILP): a scoping review. https://jfootankleres.biomedcentral.com/articles/10.1186/s13047-023-00680-6
** check out my other blog post on PAES for further information
- https://thegdphysio.co.uk/differential-diagnosis-to-calf-strain-popliteal-artery-entrapment-syndrome-paes